5. Poliomyelitis Anterior Acuta (Infantile Paralysis, Acute Atropine Spinal Paralysis).Causation
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
5. Poliomyelitis Anterior Acuta (Infantile Paralysis, Acute Atropine Spinal Paralysis).Causation
The features of this disease at the outset are those of an acute inflammation accompanied by marked general disturbance of health. These suggest a morbid poison acting on the body generally but selecting, as such agents do, a special locality for its action. Nothing is known as to the nature of the agent. The fact may be noted that the disease is much more frequent in the hotter months of the year than in the others, and it is known to occur occasionally in epidemic form. Medin expresses the belief that it is due to some infection, at present undetermined, capable of communication from person to person, although he holds that such a mode of infection is most unusual. It is a disease mostly of children, although not unknown in the adult.
The disease is an acute inflammation of the grey substance of the anterior cornua of the cord. In an observation by Drummond in which a child died after a few hours' illness, there was redness of the anterior cornua, with minute extravasations, swelling of the ganglion cells, etc. In later cases, but still comparatively early, the anterior cornua are seen under the microscope to be altered, not continuously, but in patches. They contain numerous round cells and compound granular corpuscles. The ganglion cells in certain of the groups have disappeared or have shrunk considerably. At the periphery of the affected patches round cells are aggregated, and there is already some shrinking of the patches. The condition is most manifest in the lumbar and cervical enlargements. The anterior roots are also somewhat atrophied, and show evidences of degenerative changes.
Many cases have been examined years after the onset of the disease, at intervals varying from seventeen to sixty-one years, and the changes have been very obvious even to the naked eye. These consist of sclerosis with shrinking, mainly of the anterior grey cornua, but also of the anterior and anterolateral columns of white substance (see Fig. 316). These changes are very manifest when the cord has been hardened and fine transverse sections made. The shrinking of the horn affects certain of the groups of cells specially, and the shrunken part consists largely of connective tissue in which there are visible no ganglion cells or only deformed and pigmented ones. Connective tissue with abundant nuclei and enormous numbers of amyloid bodies are visible. The lesion in the anterior cornua is by no means homogeneous or symmetrical. One cornu may be atrophied and the other normal, and on examining sections at different levels there is great variety in the longitudinal distribution. The anterior roots are also atrophied at the parts corresponding to the most affected portions of the cord, and they may appear to the naked eye small and grey.
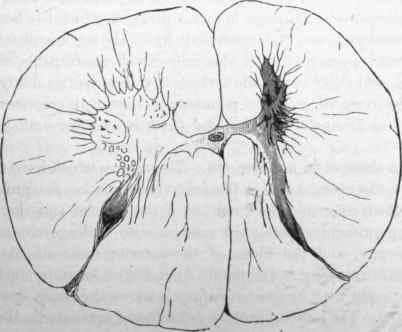
Fig. 316. - Anterior poliomyelitis. The right anterior comu in the cervical region is shrunl^en, and there is atrophy of all the white columns on that side. From a woman, aged 50, who was the subject of infantile paralysis of the right arm. (Charcot).
The disease usually begins acutely, and the paralysis generally assumes its full development almost at once. This extensive paralysis seems due in part to pressure by the distended vessels and inflammatory exudation, and in some cases by extravasated blood. In this period some ganglion cells may be destroyed, but those not absolutely destroyed may recover as the acute inflammation passes off. In many parts the inflammation is slight, and subsides completely; in others it is severe and goes on to sclerosis, and there is permanent destruction of the ganglion cells. Hence it is that a paralysis which has been at first almost universal may be recovered from almost completely. The improvement goes on till all the cells which are capable of it have recovered, and there is a residue which have been permanently lost and cannot be restored. These permanently lost cells represent single muscles and groups of muscles, and there is a corresponding localized paralysis.
Trophic Changes In Muscles, Etc
The centres which have the direct control of the contractions of the individual muscles are probably the centres which command the nutrition of the muscles and their nerves. For the permanently paralyzed muscles soon undergo *a marked and rapid atrophy, and the fibres of the anterior roots also degenerate. The muscular atrophy is not simply from disuse, for it is much greater and more rapid than in cases of paralysis where the anterior cornua are not affected. The muscles rapidly get soft and emaciated. Besides the loss of substance there may be proliferation of the nuclei of the interstitial connective tissue, and an increase in this tissue; sometimes there is infiltration of fat in the interstitial tissue, so that the muscle may appear less atrophied than it in reality is. The defective development of the bones and joints met with may be partly from disuse, but also probably to some extent from destruction of trophic centres. The bones of the paralyzed part do not grow normally, and the articulations are imperfectly adjusted. Certain deformities ensue, the commonest and most prominent of which is club-foot. Curvature of the spine is also a comparatively frequent result. All through the disease the patient may maintain good general health, and after recovery from the initial fever he may present nothing abnormal but the paralysis and atrophy. Through time he learns to use his remaining muscles to the best advantage, and may pass through a long life maimed by the infantile attack.
Although most common in children a good many cases of this disease have now been recorded in Adults. Here also it is ushered in by acute symptoms such as fever, pain in back and extremities, vomiting, headache. The paralysis develops mostly in a few hours, but it may be as late as a day or two. After a time recovery begins, and is more frequently complete than in the case of children. It is frequently incomplete, and then we have paralytic deformities, which, however, as the bones are fully formed, are not so striking as in the case of children. Here, also, there is rapid atrophy of the muscles, which is not so liable to be concealed by fatty infiltration as in the case of children.
Continue to:
My Books

