Steps In The Diagnosis And Initial Management Of The Stomach Cancer Suspect
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Steps In The Diagnosis And Initial Management Of The Stomach Cancer Suspect
Once an individual is suspected of having stomach cancer on the basis of symptoms, signs, or leads from the detection procedures outlined, there are certain diagnostic steps which are essential to the process of ruling the diagnosis in or out. Not all of them will always be required in the handling of any one patient, but each has its special contribution to make, depending on the circumstances.
The major steps to diagnosis are as follows:
1. X-ray studies (upper gastrointestinal series)
2. Cytology
3. Gastroscopy
Lesser but occasionally very helpful steps include the following:
1. Gastric analysis
2. Guaiac test
3. Hemoglobin and/or hematocrit X-ray studies
Visualization of the upper gastrointestinal tract by means of a barium meal should be the first step in the management of all stomach cancer suspects.
Indications
Indications for x-ray studies are any clinical or laboratory suspicion of gastric cancer. Parenthetically, it should not be assumed that all patients with ulcer symptoms have a duodenal lesion. A gastrointestinal series should be done at the outset to exclude the possibility of a gastric ulcer, whose potential and management may be so different.
Contraindications
There are virtually no contraindications to x-ray studies. Active gastric or esophageal bleeding or obstruction may be relative contraindications under certain conditions. Usually this means merely a delay in performing the study pending stabilization of the clinical picture (e.g., cessation of bleeding) or special preparation of the patient (e.g., gastric aspiration). In fact, many feel that a gastrointestinal series is definitely indicated in the early phases of active bleeding. Also, modifications may be introduced into the technique of the study (e.g., a thin suspension of barium) to meet special conditions. Any suggestions of intestinal obstruction, of course, demands that this diagnosis be ruled out before a gastrointestinal series is performed.
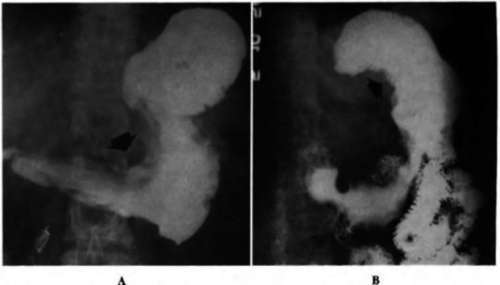
Fig. 62. A, Infiltrating and ulcerating cancer involving the body of the stomach, including the greater and lesser curvatures. B, Polypoid cancer involving the upper half of the body of the stomach on the lesser curvature and posterior wall.
Technique
The time, exacting technique, equipment, and experience required make it mandatory that such studies be done by one experienced in its performance. A casual swallow of barium followed by fluoroscopy in a patient in whom there is a suspicion of stomach cancer is to be deplored.
Findings
No attempt will be made at a detailed classification or description of the x-ray findings that can be encountered in stomach cancer. Reference to the section on the pathologic classification of lesions (pp. 175 and 176) will assist the reader in an understanding of the mechanism by which the various radiographic pictures may be produced. A relatively simple breakdown is as follows:
1. Changes in the lumen
(a) A sessile or polypoid mass lesion may be apparent.
(b) The size of the lumen may be sharply reduced by infiltration of the stomach wall with neoplasm without any specific intraluminal lesion.
(c) Obstruction or pylorospasm may cause the lumen to be enlarged or distended.
2. Changes in the mucosa
(a) Atrophy. The mucosal folds appear to be diffusely erased.
(b) Hypertrophy. The mucosal folds may be extremely prominent throughout and assume the form of giant rugae which may simulate tumor.
(c) Irregularity. A localized area of mucosal irregularity is noted.
(d) Abnormal motility. Fluoroscopic observation reveals that gastric motility is disturbed in general or, more significantly, that a wave of peristalsis sweeping over the stomach will appear to skip a localized area that is somewhat rigid and nondistensible.
(e) Ulceration. This may take the form of a simple break in the continuity of the mucosa with surrounding reaction, or it may be superimposed on an intraluminal mass.
3. Changes in the wall
(a) The stomach wall in general may become diffusely thickened, rigid, and nondistensible.
(b) The lumen may be distinctly compromised and gastric capacity reduced to varying degrees.
4. Changes in transit
(a) Obstruction. The cardia or pyloric sphincter may be partially or completely obstructed by adjacent stomach cancer. This is most commonly due to the direct local effects of the tumor but may be due, at least in part, to reflex spasm. Often the tumor itself may not be visualized at first by x-ray examination but only its obstructive effects.
(b) Atony. The stomach may lose its tone and become flaccid.
Accuracy
The accuracy of the upper gastrointestinal series in the diagnosis of stomach cancer varies widely in accordance with the size, type, and location of the lesion involved, the skill of the radiologist, and many other factors. It has been estimated that the results of a single examination done by an examiner of above-average competence in a hypothetical series of patients with stomach cancer might break down as follows:
1. 60-70% definite diagnosis of cancer possible
2. 20-25% suspicious for cancer but equivocal
3. 10-15% benign diagnosis made
4. 1-5% negative study
In all likelihood the 20 to 25? suspicious-but-equivocal studies would be repeated and the diagnosis made. But what about the close to one fifth of the patients with stomach cancer in whom the x-ray studies are benign or negative? These would probably not be repeated and the opportunity for diagnosis would have been missed. The need for keeping this figure to an irreducible minimum is obvious. Insistence on the most exacting and competent x-ray study in the first place plus prompt repeat of any indeterminate study is essential.
The need for additional diagnostic aids that complement or supplement x-ray examination and that will still further reduce the number of indeterminate cases is apparent.
Continue to:
My Books

