Other Tumors of Head and Neck
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Other Tumors of Head and Neck
Rarely occurring pulmonary tumors include the salivary gland type tumors (or cylindromas) which tend to run a malignant course and the benign hamartomas which typically present as "coin lesions."
Metastatic cancer from virtually any body site may present first as a lung tumor. The possibility of a primary focus elsewhere must always be considered when one is confronted by a suspicious pulmonary shadow on the x-ray film.
Significance Of Location Of Lesions Symptoms And Signs
In its early stages lung cancer produces symptoms and signs almost entirely on the basis of secondary effects on adjacent bronchopulmonary segments. The speed with which these develop is dependent on the location of the cancer and the size of the bronchial lumen involved. Thus a lesion may grow to a large size in a large lumen without necessarily producing any symptoms or signs. On the other hand, a small lesion obstructing a small bronchus may give rise to early clinical manifestations.
Diagnosis
The location of the primary lesion is an important determinant in the ease with which a definitive diagnosis may be reached.
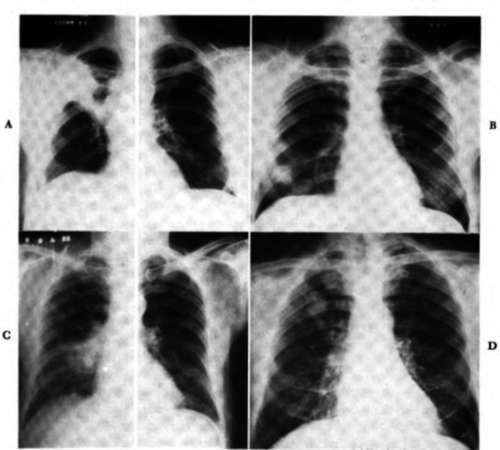

Fig. 43. Posteroanterior views of the chat. A, Note the increased density in the right upper lobe, the prominent right hilar shadow, elevation of the transverse fissure on the right, shift of the mediastinum slightly to the right, and elevation of the right leaf of the diaphragm. These findings indicate atelectasis of the right upper lobe due to a carcinoma in the right hilar region. B, Note the 4 cm. rounded infiltration in the right lower lung field. This proved to be inflammatory-benign. C, Note the 6 cm. rounded masslike infiltration associated with the right hilum with some general mild aeration loss in the right lower lung field. This is due to a proved epidermoid carcinoma. D, Note the 3 cm. rounded infiltration in the right second interspace which proved to be an adenocarcinoma of the bronchus. E, Note the 2.5 cm. ovoid density in the left lower lung field just above the diaphragm. This proved to be a bronchogenic carcinoma.
1. X-ray studies. Pulmonary cancer presents a wide range of findings radio-graphically depending upon its location and the associated changes (Fig. 43). If a tumor is located in a major bronchus, it may reach substantial size before it comprises the lumen and produces a radiographically detectable shadow; conversely, minute lesions may produce x-ray densities if they are strategically located in a peripheral bronchus. Furthermore, the location obviously determines the extent to which a lesion may be obscured by overlying heart, bone, hilum, or diaphragm-an important factor in tumors which may escape initial detection.
2. Bronchoscopy. The nearer a lesion is to the main stem bronchus, the more likely it is to lend itself to visualization and biopsy at the time of bronchoscopy. The more peripheral a lesion is, the less chance of a bron-choscopic diagnosis. Furthermore, even though a lesion is relatively central in location, if it is situated in the upper lobes, the utility of endoscopy is sharply impaired because of the technical difficulties inherent in covering the area.
3. Cytology. The tendency of neoplasms to exfoliate varies gready but, as a general rule, the more peripheral the lesion, the less the chances of a cytologic diagnosis.
Prognosis
It has already been pointed out how the location of the lesion may influence the time at which signs and symptoms occur and diagnosis is possible. Thus the stage at which the lesion is presented for surgical treatment may be determined by these factors, with its inevitable consequence on the prognosis. Beyond this, moreover, it is obvious that the location of the lesion determines whether surgery is technically feasible.
Pathogenesis
The widespread variation in the classification of lung cancer is symptomatic of a more basic lack of agreement concerning the pathogenesis or natural history of the disease. Pathologists disagree as to the exact site of origin within the bronchial mucosa, and no unanimity exists as to what cell type is the precursor of cancer. With this in mind the observations of Auerbach and associates are quite enlightening. They undertook a most exhaustive study of the tracheobronchial epithelium in a group of male adults. Specimens were obtained at autopsy or surgery, and multiple sections were taken from every ramification of the respiratory tract. The slides were carefully labeled as to origin of each specimen, and each was studied for the presence or absence of certain fairly well-defined pathologic alterations. These were noted and mapped on a chart of the tracheobronchial tree; finally, they were related to the known smoking habits of the individual. Analysis of their results showed a consistent panorama of histologic change from normal epithelium to that exhibiting stratification or basal cell hyperplasia and on to carcinoma in situ. Furthermore, there was a clear-cut relationship between the amount and degree of these changes and the smoking habits of the individuals.
Significance
1. It seems likely that there is a more or less orderly and predictable sequence of change from normal to epidermoid cancer. Malignant disease does not arise de novo; in fact, it may be incipient for a period of months or even years.
2. The close correlation of the degree and type of these changes with the known smoking habits of the individuals is further confirmation of the tobacco etiology of most epidermoid lung cancer.
3. The identification of these changes without even the slightest indication of tumor formation underscores the potential sensitivity and utility of cytology as a means of detecting and diagnosing lung cancer.
4. These changes are of diffuse character, rather uniformly distributed throughout the tracheobronchial tree. This bolsters the concept of an inhalant as a carcinogenic agent and may serve to explain why surgical attack on a single focus is often unable to eradicate the disease. What has often in the past been regarded as postoperative recurrence of the disease may, in fact, be evidence of a new primary lesion.
Continue to:
My Books

