Clinical Features In The Symptomatic Patient. Localized Lesion
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Clinical Features In The Symptomatic Patient. Localized Lesion
Although obviously there is a great deal of overlapping, the clinical features of cancer of the lower bowel can probably most conveniently be detailed by arbitrarily dividing the area into three separate regions:
1. The right colon, including the cecum, the ascending colon, the hepatic flexure, and the right half of the transverse colon
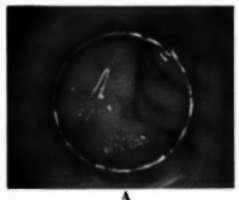

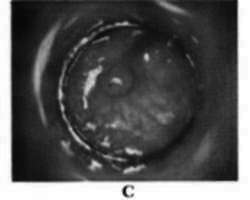

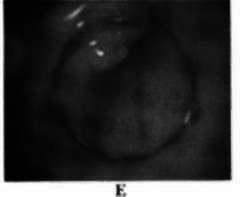
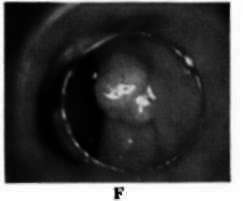


Plate 3
A, Hyperplasia. B, 4 mm. area of hyperplasia. C, 4 mm. adenoma. D, 5 mm. adenoma, E, 5 mm. adenoma. F, 1.2 cm. adenoma with beginning pedunculation.G, Pedunculated adenoma with focus of adenocarcinoma. H, Adenocarcinoma. J, Hypertrophid anal papilla. I, Lipoma.
2. The left colon, including the left half of the transverse colon, the splenic flexure, the descending colon, the sigmoid, and the rectosigmoid
3. The rectum
The anal region is not ordinarily included in this classification as a separate entity, although obviously it may be involved secondarily by lesions arising in the rectum.
Right Colon. In This Area:
1. The bowel lumen is large.
2. The stool is liquid.
3. The lesions usually grow through the wall or protrude into the lumen initially. Encircling or constricting the bowel is a later phenomenon.
4. Therefore, obstructive symptoms are unusual, and the rumor may reach a large size before causing specific complaints, particularly changes in bowel habits.
Symptoms And Signs
1. Nonspecific gastrointestinal symptoms. These may include anorexia, nausea, indigestion, abdominal distention, flatulence, etc. Right-sided abdominal pain of the type usually associated with disease of the appendix or gallbladder may be produced.
2. Anemia. Symptoms secondary to a moderate to marked anemia may be prominent (e.g., weakness, lassitude, dyspnea, palpitation, dizziness, etc.). The mechanism by which the anemia is produced is unknown. Only a small portion of it could be accounted for by bleeding, since this is seldom very marked or prominent (occult blood in the stool is often the only manifestation). The severity of the anemia by no means denotes the likelihood of inoperability in right colon lesions.
3. Abdominal mass. A right-sided abdominal mass may sometimes be palpated, since the anatomic and physiologic features peculiar to the right colon may allow a lesion to attain considerable size before declaring itself in other ways.
4. Weight loss of varying severity may be present and does not necessarily indicate a poor prognosis. Loss of twenty to thirty pounds may be the outstanding presenting symptom.
5. Others. Occasionally the first symptoms of carcinoma of the right colon, especially in the region of the cecum, may be those associated with perforation of the bowel and consequent local or generalized peritonitis plus the other manifestations of this clinical syndrome.
Sometimes the symptoms of small or large bowel obstruction may be present. If the lesion is in the region of the ileocecal valve, the clinical picture would be more consistent with the former; if in the region of the hepatic flexure or adjacent transverse colon, more consistent with the latter. With an incompetent ileocecal valve a mixed picture may be apparent.
Digital examination of the rectum and sigmoidoscopy are ordinarily unremarkable in carcinoma of the right colon.
The guaiac test will frequently be positive for occult blood. Occasionally preparation of the patient with castor oil prior to examination will result in a finding of blood or blood-tinged mucus issuing from above at the time of sigmoidoscopy.
The diagnosis of cancer of the right colon almost always rests on the barium enema x-ray examination.
Left Colon. In This Area:
1. The bowel lumen is smaller and is more easily obstructed by tumors than the right.
2. The stool is solid.
3. The lesions tend to grow around, encircle, and constrict the bowel.
4. Accordingly, obstructive symptoms of varying degree may be prominent even with relatively small lesions.
5. The function of the left colon is storage, and therefore disorders of bowel habit pattern predominate.
Symptoms And Signs
1. Change in bowel habits. An increasing tendency toward constipation may become apparent. Occasionally this may alternate with periods of apparent diarrhea. This may be very slow and insidious or develop fairly abruptly.
2. Blood in or on the stool. Frank bleeding with or without associated mucus may be present in lesions of the left colon. The degree of associated anemia, if any, is usually mild. If a more marked anemia is noted, its prognostic significance is more ominous than in right-sided lesions.
3. Obstructive symptoms. The foregoing symptoms reflect a narrowed bowel lumen due to a constricting lesion. Occasionally the situation may progress to partial or even complete large bowel obstruction, with its usual clinical manifestation.
More commonly, however, the patient complains of left-sided discomfort and distention, sometimes referred to as "gas," often crampy and episodic in character, occasionally relieved by a bowel movement or expidsion of flatus.
"Ribbon" or "pencil" stools have been described as very characteristic of left colon cancer. They may sometimes be encountered but are by no means diagnostic of such lesions.
Sigmoidoscopy and x-ray examination are of more or less equal importance in the diagnosis of cancer of the left colon. Lesions of the left half of the transverse colon and the descending colon are ordinarily accessible only to the barium enema. Occasionally blood or blood-tinged mucus may be seen through the sigmoidoscope as the only manifestation of a high-lying lesion. Uncommonly an abdominal mass may be palpated. The far more common lesions of the sigmoid and rectosigmoid can usually be seen at sigmoidoscopy if they are located within 25 cm. of the anal margin.
Digital examination is usually of little value in the diagnosis of lesions in this area.
The guaiac test will often be positive. Frequently, however, the frankly bloody nature of the stool may render this test superfluous.
Rectum. In This Area:
1. The bowel lumen is large, especially the ampulla.
2. The stool is solid.
3. The lesion tends to invade the wall and project into the lumen.
4. The function of the rectum is principally that of expulsion, and therefore disorders of the act of evacuation predominate.
Symptoms And Signs
1. Rectal bleeding. This may take the form of blood streaking or blood and mucus with bowel movements. Less commonly, frank hemorrhage of varying degrees of severity may occur at the time of a bowel movement or by itself. It may be entirely indistinguishable from the bleeding associated with hemorrhoids, and the two frequently coexist. Rectal bleeding should be attributed to hemorrhoids only after careful investigation rules out the presence of other more serious lesions.
2. Sense of incomplete evacuation. The presence of a tumor mass and/or retained feces is responsible for postevacuation fullness.
3. Tenesmus. The efforts of the rectum to expel the tumor and retained stool plus associated spasm cause the patient to experience a frequent and usually unsatisfied desire to have a bowel movement.
4. Mucus diarrhea.
5. Others. The presence of actual pain is not common in early rectal lesions unless the anal canal is involved. Obstruction is not a common phenomenon. All rectal lesions should be seen through the proctosigmoidoscope. A good number of these can also be felt with the index finger, although reliance should never be placed on this alone. X-ray examination is ordinarily of little value in the diagnosis of rectal cancer. In fact, it can be dangerously deceptive.
Although the transverse colon is not ordinarily treated as a separate entity when speaking of large bowel cancer, a few words about its characteristics might not be amiss.
1. It is a zone of transition from the right to the left colon.
2. Symptoms and signs of one or the other side may be dominant, depending on proximity of the lesion to the hepatic or splenic flexure.
3. The bowel lumen is of intermediate size.
4. The stool is of semisolid consistency.
5. Because of its relatively superficial location, a rather small mass may be palpable.
6. Because of its rather strategic location, a relatively early lesion may invade contiguous structures (e.g., stomach).
Advanced Lesion
As a rule, it is unwise to be overly dogmatic about classifying a case of cancer of the rectum and colon as "early" or "late" on the basis of symptoms and signs. Such a judgment may have its pitfalls even when the operative findings and pathologic sections are available for consideration. A very large lesion with a long clinical history and apparent evidence on physical examination of invasion and fixation of adjacent structures may prove to be quite well localized and without metastasis. The fixation of contiguous tissue may be purely inflammatory rather than malignant.
The degree of anemia and the amount of weight loss have already been mentioned as uncertain indicators of long-range prognosis.
However, the following can be said:
1. Evidence of distant metastasis makes a classification of "late" or advanced mandatory.
(a) Enlargement and nodularity of the liver on physical examination, with or without ascites and jaundice
(b) X-ray evidence of metastasis to the lungs or, much less commonly, to the bones
(c) Enlargement of distant lymph nodes, especially left supraclavicular (Virchow's node) and axillary
2. Evidence of local progression, invasion, and spread to contiguous or nearby structures makes a classification of "late" presumptive or at least possible.
The clinical features characterizing the advanced lesion, which are more or less peculiar to carcinoma of a specific area, are as follows:
Right Colon And Transverse Colon
1. Perforation
2. Fixation to liver or gallbladder, stomach, pancreas, or small bowel
3. Adherence to anterior abdominal wall
4. Gastrocolic fistula
Left Colon And Rectum
1. In women: invasion of female pelvic organs, rectovaginal fistula, seeding of ovary (Krukenberg tumor)
2. In men: spread to prostate gland
3. Invasion of small bowel, bladder; obstruction of ureters
4. Vesicocolic or rectovesical fistula
5. Spread posteriorly to sacrum and adjacent nerve structures
6. Rectal shelf (Blumer's) mass
7. Enlargement of inguinal nodes, especially bilateral
8. "Frozen pelvis"
Generally speaking, in the absence of definite distant metastases, most lesions of the rectum and colon are considered operable. It is true that a substantial number will prove to be nonresectable for cure. Such a judgment, however, is often possible only on the basis of the findings at operation and subsequent pathologic study. Moreover, a palliative resection is frequently required for symptomatic relief.
Continue to:
My Books

