XI. Tumours Of Bone
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
XI. Tumours Of Bone
The tumours of bone spring from the active tissue which enters into the composition of bone, and this has been shown to be, on the one hand, the medulla, forming not only the marrow of the long bones, but occupying also the spaces of the spongy bone and the various canals of the dense bone; and, on the other hand, the subperiosteal layer, which really is formed of the same tissue as the medulla. The tumours of bone may be distinguished according as they arise from the medulla, in which case they may be called Central or Myelogenous, or from the subperiosteal layer when they Are designated Peripheral or Subperiosteal. Originating in these structures the tumours of bone very frequently contain bone which is produced by a process of new-formation in the tumour itself. This applies more particularly to the fibrous, cartilaginous, and sarcomatous forms, but even in cancers there is sometimes an ossification of the stroma.
The primary tumours of bone belong to the connective tissue series, but from the near connection of some of the bones (especially the jaws) with epithelial structures, we may have tumours composed of epithelium, such as cysts and cancers, as primary tumours involving the bone. Of the typical tumours the commonest are the Osteoma, Chondroma, and Fibroma, while the Myxoma, Lipoma, and Angioma constitute rare forms. Amongst the atypical, Sarcoma in various forms is somewhat common as a primary tumour, while Carcinoma is frequent as a secondary growth. Cysts are frequent in the bones of the jaws.
Osteoma
The osseous tumours in connection with bone have been distinguished as exostoses when they grow on the surface, and enos-toses when they are central. The former are much the commoner. According to structure they are designated ivory exostoses when they •are composed of dense bone, and spongy exostoses when of cancellated bone. In some of the exostoses the bone is formed from membrane, in others from cartilage, so that a layer of cartilage covers the surface of the tumour so long as it is growing. This form is sometimes called the Cartilaginous exostosis. (See p. 220).
It may be added that Multiple exostoses are of occasional occurrence. In the case from which Fig. 289 is taken (Virchow) the patient, a boy ten years of age, had suffered, during the course of three years, from repeated attacks of rheumatism affecting the joints and muscles. The result was the formation of sixty-five exostoses on various bones of the body. Exostoses also occur not infrequently at the insertion of tendons, growing into the latter and sometimes even separate from the bones. These are connected in their origin with the contraction of powerful muscles, occurring chiefly where such muscles are inserted, and sometimes induced by specially violent exercise of the muscles.
Fibroma
These tumours are mostly peripheral, but they have been observed also centrally in the lower jaw, vertebras, and ends of the long bones. The peripheral ones mostly occur in the bones of the face and cranium. They sometimes grow into the nares, forming nasopharyngeal polypi. In structure they consist of an intricate mesh-work of fibrous tissue. They do not form limited tumours, but grow out from the periosteum over a considerable area, and are • firmly adherent to the bone. Trabecule of bone frequently traverse the tumour tissue.
Chondroma
This occurs both as a central and as a peripheral tumour. The characters of the cartilage vary somewhat in different cases.
The central chondromata originate in the medulla, especially in the small bones of the hands and feet, and they are often multiple. They may grow till they distend and even rupture the bony shell (see p. 218, Fig. 74).
The peripheral chondromata occur on the long bones, the bones of the trunk, and those of the head. They are generally nodulated.
The name Osteoid chondroma has been given by Virchow to a form of tumour which merits a more special description. The tumour is composed essentially of tissue such as we find in the deep layer of the periosteum of a growing bone, or in callus, its main constituents being osteoblasts. The cells are smaller than cartilage cells and mostly round; they do not possess capsules. There is a dense intercellular substance which has a somewhat fibrous appearance. In the midst of the tissue portions of true cartilage may be found. Being formed of tissue analogous to that which is preliminary to ossification it frequently undergoes calcification and even conversion into true bone.

Fig. 289. - Multiple exostoses of femur, tibia, and fibula. These are grouped towards the ends of the diaphyses. At its lower end the fibula is flattened by the exostoses growing out from the tibia. From a boy ten years of age. One third the natural size. (Virchow).
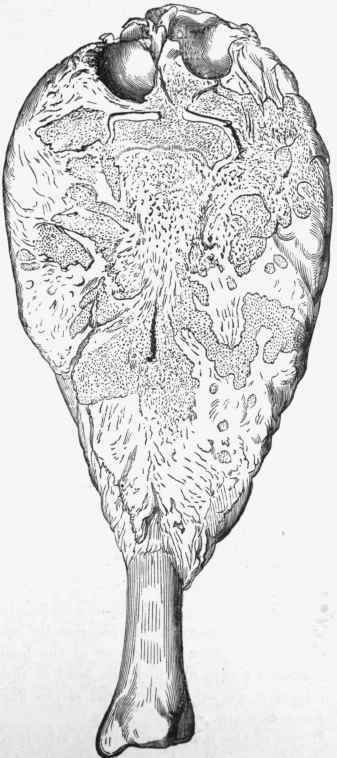
Fig. 290. - Osteoid chondroma of the tibia, divided obliquely. At the upper extremity the tumour has surrounded the cartilages of the knee, and new-formed cartilages have been produced. Internally the bone is condensed by the new-formation of bony masses. From a boy 13 years of age. (Virchow).
Such tumours form, mostly, under the periosteum of the long bones, and their seat of election is the lower end of the femur or the upper end of the tibia, originating probably in the layer of osteoblasts there, and they may grow to large dimensions. They thus form club-shaped expansions of the long bones (Fig. 290). On section the tissue is found to be dense, and it becomes osseous or calcareous on passing deeply, where it is incorporated with the bone. The medullary cavity of the bone is often filled with new-formed bone. This form of tumour sometimes presents a tendency to become sarcomatous, and even without that it may recur after removal.
Continue to:
My Books

