3. Cancers Of The Uterus And Vagina
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
3. Cancers Of The Uterus And Vagina
In the great majority of cases the cancer begins just about the junction of the uterus and vagina, and involves both as it extends. The disease scarcely occurs before the age of thirty, and is most prevalent between forty and fifty. It appears also from the statistics of West that, contrary to what is sometimes stated, it occurs much more frequently in women who have borne children than in those who have not, and most frequently in those who have had more than the usual number of pregnancies; it is as if the disease developed most readily when the uterus is deteriorated by repeated conceptions.
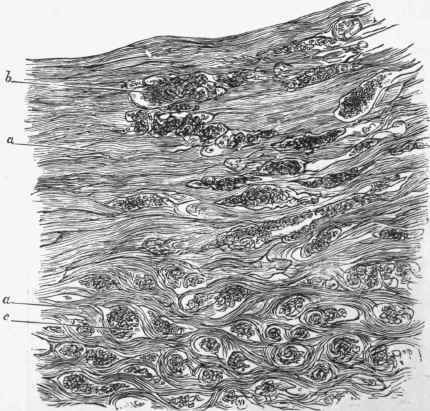
Fig. 456. - Section of cancer of uterus under a very low power, showing mode of advance into wall of uterus, a, muscular substance of uterus, interrupted frequently (as at 6) by masses of cancerous structure. At lower part of figure (at c) the muscular substance is still more frequently interrupted and the tissue has quite an alveolar appearance, the muscle partly forming the stroma, x 22.
The cancer mostly consists of large flat epithelial cells, and in most cases these insinuate themselves amongst the constituents of the uterine wall, while in some cases the growth is more superficial. Hence it is possible to distinguish an infiltrating from a superficial form, the latter being frequently designated Epithelioma.
Infiltrating cancer begins as an infiltration of a limited part of the portio vaginalis, and extends more or less round the external os. By and by the whole portio vaginalis is converted into a hard, irregularly prominent tumour. At first the infiltration is confined to the mucous membrane and submucous tissue, but by degrees it spreads both deeply and laterally. It insinuates itself into the muscular substance of the uterus, separating and breaking up the muscular trabecule, which come to form a kind of rough stroma for it (see Fig. 456). It also passes into the vagina, infiltrating its wall. Very soon ulceration of the surface sets in, and in its subsequent course there is a progressive ulceration and infiltration, the former following the latter. The infiltration passes into the body of the uterus, but does not usually reach the fundus before the death of the patient. If the parts be examined post mortem (Fig. 457), it will be seen that an irregularly excavated ulcer occupies the adjacent parts of the uterus and vagina, rendering their respective limits inappreciable. Then, outside this, there is the whitish cancerous tissue, which extends into the uterine substance some lines beyond the ulcer.
This disease affects neighbouring structures. There are cancerous masses usually in the ligaments and under the peritoneum. The bladder is frequently adherent to the uterine cancer and its mucous membrane red and irregular, or else it presents cancerous nodules. The ulceration even extends sometimes into the bladder, which forms thus a communication with the vagina. The rectum is much less closely related to the cervix uteri than is the bladder, and it is less frequently involved. Those parts of the uterus which are not engaged in the cancerous disease are inflamed, and adhesions are formed to the rectum and urinary bladder. Although thus extending locally, the cancer has little tendency to form secondary tumours in the lymphatic glands, and still more seldom does it become generalized.
It sometimes happens that the new-formation of cancerous tissue is more vigorous than the ulceration, and in that case we may have prominent ragged masses hanging into the vagina.
The microscopic examination of this form of cancer shows masses of epithelial cells, usually of considerable size, arranged irregularly in the alveoli, the stroma being largely formed by the remains of the struc tures into which it has infiltrated.
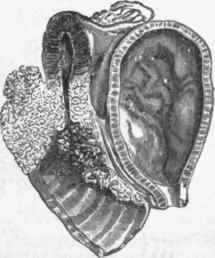
Fig. 457. - Ginccr of uterus, the parts shown in section. To the right is the. urinary bladder. To the left are vagina and uterus, both of them to a large extent converted into irregular cancerous masses. (Graily Hewitt from Martin).
Epithelial cancer (Cancroid) is hardly to be distinctly delimited from the former, but is characterized by a more superficial outgrowth of prominent warty projections, while the deeper infiltration is slower and less in degree. The disease begins, as in the other case, in the portio vaginalis, and at first there is little more than a prominent warty outgrowth. But the warty growth increases while the base becomes infiltrated till a bulky prominence results, whose surface, consisting of masses of papilliform projections, gives the character of the Cauliflower excrescence (Fig. 458).
This form of tumour is also liable to ulceration, and there may be a combination of ulceration with papilliform projections, although, after a time, the papillae may be destroyed and the appearances approximate to those of the other form of cancer.
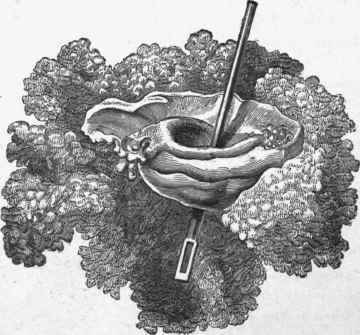
Fig. 458. - Cauliflower cancer of posterior lip of os uteri. A probe is passed through the os, and the anterior lip in front of it is seen to be normal, while a cauliflower growth projects from the posterior. (Simpson).
Under the microscope the structure here is more that of flat-celled epithelioma. The prominent papillae are covered with pavement epithelium, and the deeper infiltration consists of masses of flat cells.
A few cases have been observed in which Colloid cancer has been the form occurring in the uterus, the situation being the same as in the other more common forms. In rare cases also a cancer may arise from the fundus uteri.
Continue to:
My Books

