2. Pigmentation By Haemoglobin And Its Derivatives
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
2. Pigmentation By Haemoglobin And Its Derivatives
The pigment of the red corpuscles of the blood, the haemoglobin, is an unstable substance, and rapidly passes into other forms. Haemoglobin contains iron, but the latter is so intimately combined that it does not give the usual reactions of iron, such as that with ferrocyanide of potassium and hydrochloric acid, unless the haemoglobin be first decomposed. The haemoglobin next yields a pigment in which the iron is loosened from its combination, and is detectable as iron. This substance has been called, by Neumann, hemosiderin. The next stage is that the pigment loses its iron, and, still retaining its red colour, is transformed into hsematoidin, which does not contain iron. This substance occurs in granules, but also in the characteristic crystalline form already figured. Haematoidin is identical with the biliary pigment bilirubin in its composition and in the form of its crystals. Haemin, which is procurable artificially from blood, has crystals presenting similar angles <Fig. 48).
In haemorrhages the tissues around usually become stained, and the pigmentation, with various alterations, may remain for years. There are two different ways in which the pigmentation may occur. In the first case the haemoglobin gets dissolved out of the red corpuscles, and the coloured solution stains the tissues around. The dissolved pigment may be transformed into haemosiderin, and the ferrocyanide test will give a general blue staining. The pigment is then liable to be collected in cells, where it may assume a granular form. The hemosiderin then passes into haematoidin, or there may even be a more direct transformation into haematoidin, which again is a much more stable product. The haematoidin occurs either as granules or crystals.
The other mode of pigmentation in haemorrhage is that the red corpuscles are taken up by amoeboid cells and their pigment undergoes transformation inside the cells. The effused blood acting as an irritant induces inflammation around, and the usual amoeboid cells, acting as phagocytes, take up the red corpuscles. (See Fig. 49.) Many of these cells pass off by the lymphatics, but some may remain permanently in the 'part. The red corpuscles inside the cells shrink, and their pigment goes through the transformation into haemo-siderin and haematoidin.
In some chronic inflammations there is a pigmentation which presumably arises in a similar way to that described above, the haemorrhage being by diapedesis. This pigmentation is met with chiefly in the skin and the intestine. There is a similar pigmentation in passive hyperaemia, due to haemorrhage by diapedesis. This is seen in the lungs, where we have the condition of brown induration, and in the liver where passive hyperaemia is usually associated with pigmentation of the hepatic cells.
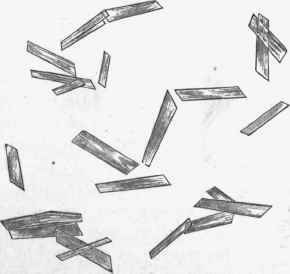
Fig. 4S. - Crystals of haemin prepared artificially by adding glacial acetic acid to a drop of blood, heating and evaporating to dryness, x 350.
Post-mortem pigmentation of the tissues should be carefully distinguished. After death dissolution of red corpuscles occurs as a result of putrefactive changes, and the pigment set free stains the tissues, more particularly the walls of the heart and vessels, but, by degrees, other structures also.
Melanaemia is a name given to cases in which free pigment is present in the blood, being the result of the destruction of the red corpuscles by the parasites of malarial fevers. The pigment is in the form of granules and flakes, and being deposited in certain organs leads to a coloration of them. (See further on).
We frequently meet post-mortem with a black pigmentation, more particularly in the mucous membrane of the intestine, but also in other of the organs in the abdomen. This is partly a post-mortem appearance, but it owes its occurrence to conditions which have existed during life. The name Pseudo-melanosis has been applied to it. Its existence implies the presence of hasmosiderin, and the black colour is due to the action of sulphuretted hydrogen evolved by the putrid decomposition, on the iron of the hremosiderin. It is thus an evidence of the presence during life of chronic inflammation, passive hyperemia, or other cause of the occurrence of hsemosiderin.
Continue to:
My Books

