Chapter XXX. Massage Treatment For Disorders Of The Respiratory System
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Chapter XXX. Massage Treatment For Disorders Of The Respiratory System
In nearly every book on massage much space is devoted to the treatment of scoliosis and similar deformities. Not so here, however, as massage for these cases is of small service. The remedy consists of exercises with which the present work does not pretend to deal. As stated in the preface, though it is well to emphasise it once again for fear of misrepresentation, I have only attempted in these pages - with rare exceptions - to indicate how the movements of massage should be performed, what effects we may reasonably expect to secure as the result of these movements, and what our aim should be when called upon to treat various conditions. When "exercises" have been described it has been my aim to fill the gaps that appear to me to exist in many of the ordinary text-books.
As already stated over and over again, massage is merely a means to an end, and that end is restoration of function. If it is true that "movement is life," massage alone as a remedial agent can rarely, if ever, suffice to cure. It can prepare the way for, and can assist in, the performance of the one and only means by which function can be fully and finally restored - the prescription and performance of suitable exercises. It is impossible to record these here, for they cover the whole realm of Swedish educational and remedial exercises.
Massage pure and simple plays but a small part in the treatment of deformities of the chest or of diseases of the respiratory system. They can therefore be dismissed in a few words.
Laryngitis, even in its acute stage, is amenable to massage treatment; in the chronic stage great benefit can be bestowed on the patient. The ordinary "clergyman's sore throat" is purely due to posture. The barrister, who always speaks with his chin raised to an audience placed above him, never suffers from any vocal effort. Many clergymen who address their congregations from a pulpit do so. Keith has assured us that the human larynx could not have been perfected without the assumption of the upright attitude. As a prophylactic, then, it is our duty to teach anyone who has to strain his voice, to do so with head well thrown back, and no evil will follow even prolonged strain. Those who cannot learn this trick can derive the utmost benefit if we teach them to stroke their own necks downwards for a few minutes after every occasion on which they are called upon to do much speaking.
In all cases of acute laryngitis - except, of course, in septic cases such as those of Ludwig's angina, when massage is strongly contra-indicated - great relief follows rhythmical down stroking of the neck (see Figs. 131 to 133, p. 297). The seance should be short, not lasting more than eight or ten minutes.
Massage treatment in acute bronchitis can rarely, if ever, be advocated. It might be possible to assist the expectoration of "sticky" mucus by very gentle hacking over the apices and the back. The clothes should not be removed, as no exposure whatever is permissible. Massage treatment of the head and neck would help a patient who was suffering from insomnia.
In chronic bronchitis there is almost always a certain amount of chronic over-distension of the air-spaces of the lungs. Thus the treatment of chronic bronchitis may be considered together with that of emphysema.
Mont-Dore is the elysium of sufferers from these complaints. The treatment consists of douche treatment applied to the thorax, and subsequent inhalation; the amplitude of respiratory movements is definitely increased thereby. But, as Graham points out, massage treatment is of far greater general application, and is available for those who cannot visit the South of France. Moreover, he quotes cases to prove that massage alone can very nearly equal the douche in improving respiratory movement. So, when we remember that to massage movements proper we can add compression movements and exercises, it would seem that much can be done to aid patients in their own homes.
Local massage treatment should consist of deep stroking and kneading of the intercostal muscles and of percussion over the apices and back - the former for the amelioration of the actual chest movements, and the latter to loosen mucus.
It is well to remember that the emphysematous patient can rarely take adequate exercise, and that often the heart is enlarged. Treatment should therefore follow closely on the lines laid down in the previous chapter when dealing with disorders of the heart. The right side of the heart is the one that suffers most in these cases, and so there will be definite indication for abdominal massage, designed particularly to assist the portal circulation. Many of the patients will be found to suffer from flatulence, so massage of the colon will frequently be indicated; many also are obese, and appropriate treatment should be added. But the real agent through which alleviation comes is exercise, suitably designed and adequately taught. Massage can prepare the way; in no case can it supplant treatment by exercises.
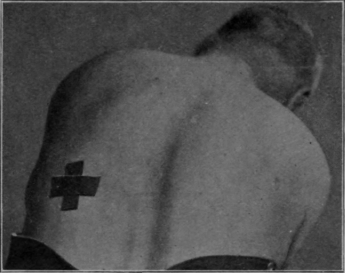
Fig. 150. - To illustrate the position for a special breathing exercise when the patient has suffered from a left-sided empyema. The hand of the masseur is placed over the area marked by the cross, and the patient endeavours to push the hand away during inspiration.
Little can be done to aid the sufferer from bronchiectasis by massage; but it would always be kindness to instruct parents to administer mild hacking and clapping over the bases of the lungs during the morning evacuation of pus. It might well hasten this most unpleasant process.
Graham reports a paper published by Schlegel advocating the use of percussion in cases of pleuritic effusion. For this purpose the ulnar border of the hand was used striking at the rate of two blows per minute" for five minutes, two seances being given daily. Non-infected pleuritic effusion is usually absorbed without difficulty. Failing this it can be relieved by tapping. If it were infected, percussion could hardly assist in the cure. It is not likely, therefore, that we shall be asked to deal with any case of pleurisy. It is a fact that there is some connection between the surface of the chest and the lungs, and it is possible that the pain of pleurisy might be alleviated by frictions over the intercostal muscles. On auscultation it is usual for the patient to complain that some spots are tender when touched by the stethoscope. Friction gradually approaching these points might well afford relief by reflex.
The treatment of the sequalae of empyema is almost entirely a question of exercises. They should be designed to mimic as far as possible Abbott's treatment for scoliosis by means of the plaster-jacket. In other words, the patient should be taught to expand the base of the lung of the side affected, when, by posture, the chest wall over this area is submitted to the fullest degree of tension that is possible. Thus, for a left-sided empyema, the patient is placed in the lax-stoop-sitting position. The trunk is then rotated to the right and the forward bend is accentuated. A hand is now placed over the left lower ribs behind, and the patient is instructed to try to push the hand away during inspiration (see Fig. 150). Other remedial and educational exercises should be prescribed as the nature of the case permits. Particularly valuable among the former are lateral costal breathing and one-sided breathing exercises, arranged in order of progression. Blowing a child's windmill is an excellent exercise.
Massage treatment, if required, should be purely symptomatic. There are no definite indications.
Continue to:
My Books

